Hospital medicine groups are frequently evaluated based on the total length of a patient’s hospital stay, even though portions of that stay occur before the patient reaches hospital medicine. This misalignment makes it hard for teams to understand their true impact on throughput and care progression. This blog explains the importance of measuring hospital medicine-specific LOS, the data needed to evaluate it accurately, the biggest operational culprits driving delays, and how technology like Medaptus Assign helps ensure patients are seen on time, workloads are balanced, and LOS is reduced.
At the end of the day, every patient in the hospital wants the same thing: to go home. The reality of getting patients home, safely and healthy, is not as simple as it seems. There are many pieces of the puzzle that impact length of stay – and cause patients to stay in the hospital longer than necessary. At medaptus, we’re one piece of the puzzle that can help patient throughout and ultimately achieve your goal: get patients out the door, safely.
Let’s dive into:
- Why Length of Stay Matters in Hospital Meidicne
- Why Total LOS is the wrong metric
- How to calculate Hospital-medicine specific LOS
- Operational causes of LOS
Why Length of Stay Matters in Hospital Medicine
Why should hospitalists care about length of stay beyond hospital leadership asking for it? For hospitalists, improving LOS directly affects how manageable daily patient care becomes. Let’s focus on three impacts:
- Hospitalist workloads and resources
- Bed availability and patient throughput
- Financial implications
1. LOS Directly Impacts Hospitalist Workload
When patients remain hospitalized longer than necessary, the hospital medicine census grows. This creates a cascading workload effect for providers and the broader care team.
Every additional day consumes a combination of staff time, equipment, and clinical resources:
- Staff resources (Another physician evaluation, additional nursing care, case management coordination)
- Equipment (Pharmacy and medication administration, IV pumps, monitoring devices, beds)
- Documentation and order management
Over time, prolonged stays can lead to:
- Larger provider census
- Increased rounding times
- Delayed discharges
- Provider fatigue and burnout
When patients remain hospitalized longer than clinically necessary, these resources stay tied up and become unavailable for new admissions.
Improving LOS helps hospitals maintain smoother patient flow and more sustainable staffing workloads.
Reducing avoidable LOS allows hospital medicine teams to manage more predictable patient volumes and focus attention on active clinical needs rather than prolonged inpatient monitoring.
2.LOS Influences Bed Availability and Patient Throughput
Bed availability is one of the most critical operational challenges hospitals face. When beds remain occupied longer than necessary, incoming patients must wait for care.
This leads to:
- Emergency department boarding
- Delayed transfers from ICU or procedural areas
- Reduced ability to accept new admissions or transfers
Hospital medicine teams play a key role in maintaining patient flow by progressing care efficiently and identifying discharge readiness early.
Earlier discharges help ensure beds are available for new patients who require inpatient care, improving the hospital’s overall throughput.
3.LOS Has Direct Financial Implications for Hospitals
Most inpatient hospitalizations are reimbursed under Diagnosis-Related Groups (DRGs), where hospitals receive a fixed payment for the entire stay regardless of the number of days a patient remains hospitalized.
This means that each additional inpatient day increases hospital costs without increasing reimbursement.
Generally:
- The first days of a hospitalization are the most resource-intensive and financially aligned with reimbursement.
- Additional days often generate incremental cost without additional payment.
When LOS extends beyond the expected DRG benchmark, hospitals may experience reduced margins for that admission.
Efficient LOS management allows hospitals to maintain financial sustainability while still delivering high-quality care.
Because LOS affects workload, hospital capacity, and financial performance, accurately measuring the portion of LOS hospitalists actually control becomes essential. Without that visibility, it is difficult for hospital medicine leaders to identify where operational improvements are truly needed.
Measuring Length of Stay
Most hospitals measure Length of Stay (LOS) using a very simple formula: LOS = Discharge Date/Time – Admission Date/Time.
The admission timestamp typically starts when:
- The inpatient admission order is placed, or
- The patient is formally admitted in the ADT system.
This means LOS includes time spent in:
- Emergency Department boarding
- ICU prior to transfer
- Procedural recovery areas
- Bed placement delays
This is why hospital medicine teams often inherit LOS time before they ever see the patient.
Hospital Medicine Length of Stay vs. Overall Length of Stay
In most hospitals, LOS starts the moment an inpatient admission order is placed—even if the patient remains in the ED or ICU for hours before the hospitalist team assumes care.
Many hospital medicine teams are held accountable for length of stay metrics – and get flagged if patients are staying longer than what is typical for that diagnosis. The problem, is that length of stay can include many things that the hospital medicine team can’t control – such as how long they were in OBS, delays waiting for a surgery, or once a discharge is medically appropriate but discharge paperwork and post-stay clinical plans are delayed. Hosptialists end up accountable for time they didn’t influence. By the time a hospitalist receives a patient assignment, several hours of LOS may already be accumulated due to ED boarding or transfer delays.
Ideally, as a hospital medicine team, you want to drill into the hospital’s overall length of stay and understand what the hospital medicine length of stay is specifically, and for each diagnosis. This may be called “attributable OS” or “provider-controlled LOS.”
The Best Way to Measure Hospital Medicine Length of Stay
There are a few common approaches used by operational leaders:
Option 1 — Assignment Timestamp (Most Accurate Operationally)
Hospitalist LOS = Discharge Time – Patient Assignment Time
Benefits:
- Reflects the moment the team takes responsibility.
- Captures operational workflows hospitalists influence.
Option 2 — First Encounter Timestamp
Hospitalist LOS = Discharge Time – First Provider Encounter
Downside:
- Documentation delays skew the number.
Option 3 — Bed Transfer to Floor
Hospitalist LOS = Discharge Time – Floor Arrival
Downside:
- Not all patients go to floors immediately.
If you want to truly capture what hospitalists can control, then option one is the best choice.
Now that we’ve discussed why length of stay is important and how to measure it, let’s discuss what contributes to a high length of stay.
What Is Actually Within the Hospitalist’s Control?
Not every driver of length of stay is operational. Many patients remain hospitalized longer simply because they are medically complex or require extended treatment.
However, several factors that influence LOS are tied to care coordination and clinical workflow within the hospital medicine team’s control.
Continuity of care is one of the most important. When a patient remains under the care of the same hospitalist throughout their stay, decisions tend to move faster because the provider has full context on the patient’s history, treatment plan, and discharge readiness. When care frequently shifts between multiple physicians, nurses, or consulting teams, providers often need to re-review the case, verify prior decisions, and rebuild the clinical narrative before progressing care.
Shift transitions can also introduce delays. When a hospitalist is nearing the end of their shift, there is often a strong incentive to complete discharges before handing the patient off to another provider. If a patient instead transfers to a new physician late in the day, the incoming provider may take additional time to confirm the treatment plan before proceeding with discharge, which can unintentionally delay the patient’s departure by several hours—or even an additional day.
Hospitalists must also carefully balance discharge timing with the risk of readmission. Hospitals closely track readmissions as a quality and financial metric, and discharging a patient prematurely can result in avoidable returns to the hospital. In some cases, keeping a patient an additional day for stabilization or care coordination may ultimately prevent a readmission and improve overall outcomes.
For hospital medicine teams, the goal is not simply to discharge patients as quickly as possible, but to coordinate care efficiently, maintain continuity where possible, and ensure patients leave the hospital safely and at the appropriate time.
Understanding which LOS factors are clinical realities and which are operational inefficiencies is critical. Without that distinction, hospital medicine teams may be held accountable for delays they cannot influence while missing opportunities to improve the workflows they can.
Once hospital medicine leaders understand which factors truly influence hospitalist-controlled length of stay—such as patient visibility, balanced workloads, and continuity of care—the next step is implementing workflows that support those goals. Technology like Medaptus Assign helps operationalize these processes by ensuring patients are assigned quickly, workloads remain balanced, and teams maintain continuity across shifts.
How Assign Helps Hospital Medicine Teams Improve LOS
Our automated patient assignment software, Assign, helps hospital medicine teams be set up for success to ultimately improve length of stay.
- We improve care continuity by automatically assigning patients to the same provider who cared for them the previous day whenever possible. Maintaining consistent provider assignments reduces unnecessary handoffs, limits repeated chart reviews, and allows clinicians to progress care more efficiently because they already understand the patient’s clinical history and treatment plan.
- Assign also helps balance workloads across the care team. Rather than relying on manual or ad hoc patient distribution, the platform ensures providers receive a more even mix of new admissions and existing patients. When workloads are distributed more equitably, hospitalists can round earlier, make clinical decisions sooner, and avoid delays caused by overloaded providers.
- In addition to improving day-to-day workflows, Assign gives hospital medicine leaders more accurate insight into their performance metrics. The platform helps identify and remove outlier cases—such as unusually long hospitalizations driven by extreme clinical complexity—from LOS reports (for example, exclude any stats greater than 12 days). This allows leaders to focus on trends they can realistically influence rather than having performance metrics skewed by rare but unavoidable extended stays.
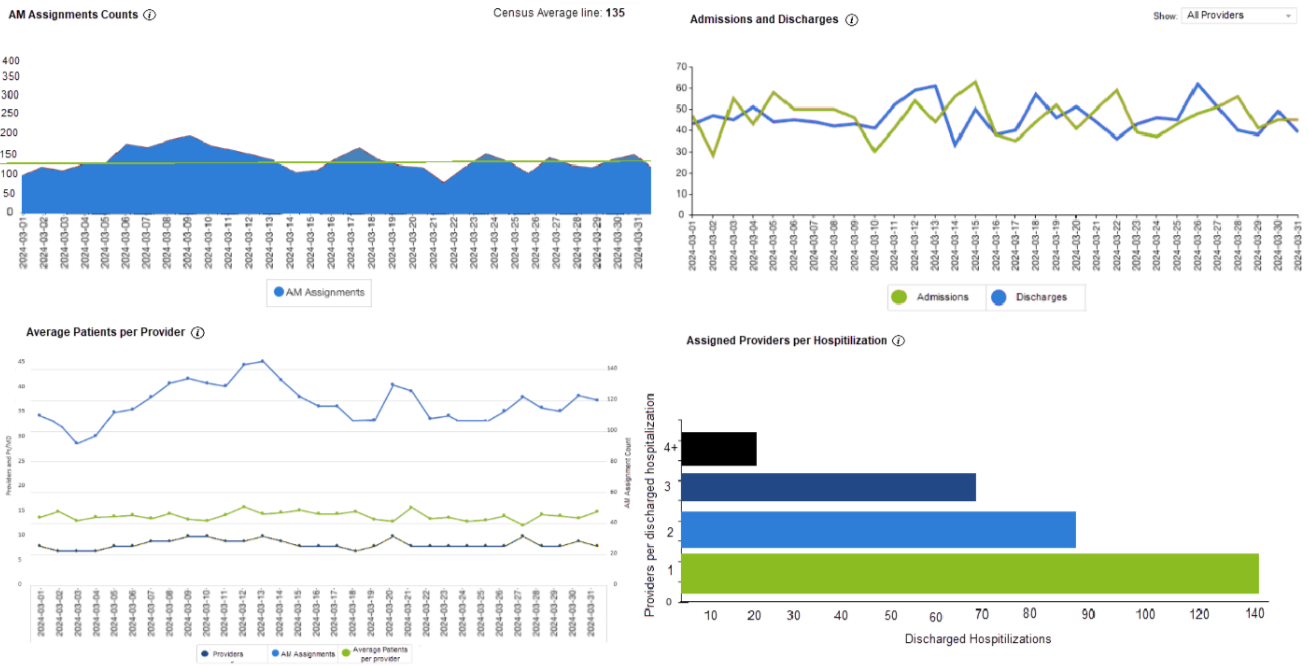
- Measure what matters. Using our Hospital Medicine Analytics, you can dive into reports that can help you understand operational bottlenecks before they happen. For example, our Assigned providers per hospitalization report shows you how many providers saw a patient in their hospitalization – fewer providers correlate to a shorter length of stay.
Together, these capabilities help hospital medicine teams maintain continuity, improve operational efficiency, and gain clearer visibility into the portion of length of stay they can actually control.
Final Notes
Length of stay will always be influenced by many factors across the hospital, but hospital medicine teams should be measured on the portion they can realistically control. By isolating hospital medicine–specific LOS and focusing on workflows like timely patient assignment, balanced workloads, and continuity of care, leaders can gain clearer insight into where improvements can be made. When hospital medicine teams are empowered with the right metrics and operational tools, they can focus on what matters most—progressing care efficiently and helping patients return home safely.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.