

Blog Summary
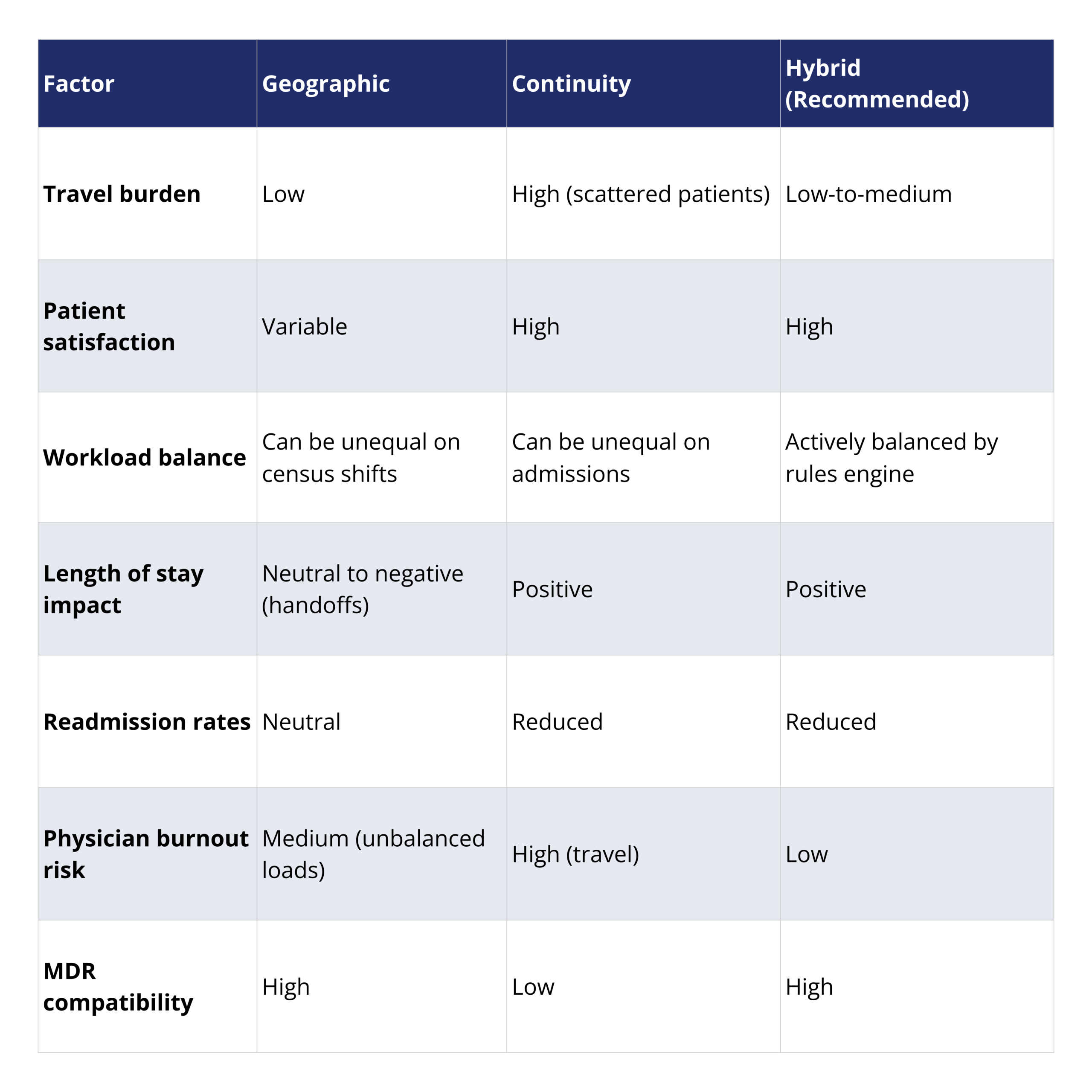
Neither pure geographic rounding nor pure continuity of care rounding is optimal on its own. The best hospitalist patient assignment model is a hybrid: patients stay with their assigned physician as long as they remain within a defined geographic zone (e.g., same floor or tower), but are reassigned when they move significantly. This approach improves workload balance, reduces physician burnout, lowers length of stay, reduces readmission rates, and improves patient satisfaction — outcomes supported by clinical research. Implementing this hybrid model effectively requires automated patient assignment software that can enforce these rules dynamically throughout the day.
The struggle between Geography and Continuity within a hospital setting is a conundrum that still hasn’t been settled by today’s hospitalists. Over the past 20 years, we have worked with many different patient assignment workflows ranging from smaller hospitals to large health systems all over the country. In working with these different groups, we’ve come to realize it’s not so much about geographic rounding vs. continuity rounding, but rather an optimal balance between the two that allows for continuity of care but does not sacrifice the benefits of geographic based rounding.
In this blog, we will speak to these two philosophies first and then discuss the balance that needs to be served between the two.
How Should Hospitalists Balance Geographic Rounding and Continuity of Care?
What Are the Benefits and Challenges of Geographic Patient Assignment?
First off, geographic patient assignment on its face is a straightforward simple approach. We can break it down like this:
- Our sample hospital has 10 floors, each floor has two units (units A and B).
- Hospitalist teams are assigned 1 hospitalist to 1 unit on a floor each day.
- Hospitalist A is working floor 9 unit A of the hospital.
- As patients are admitted or transferred to floors, they are now the responsibility of the rounding provider assigned to the floor.
Easy right? Here’s an example of a problem that could arise. I had started my week with 15 patients all located on floor 9 unit A of the hospital. Let’s say, on the 3rd day of my 7-day shift, 3 patients have now been transferred to the 2nd floor on unit B. I’ve been rounding on those patients for the past 2 days. Should I keep those patients still? How does that affect my overall rounding workload? How much time does it take me to get to the other floor? What if on the 4th day of my shift, another patient is transferred to the 8th floor, unit A, which is very close to where I am doing my rounds, however, there is another provider working that floor, should we switch care of the patient? Let’s say on the 5th day of my shift, I have 4 patients that came into the hospital overnight and plans to be admitted to the 9th floor, unit B, however, they have not been seen by the overnight nocturnist doing admissions. I now have an unbalanced rounding workload compared to my colleagues because of all the new admissions.
All these situations occur over the span of a rounding stretch. Traveling large distances back and forth to see patients and unbalanced workloads can lead to physician burnout. Attempting to keep geographic rounding intact throughout the shift can also cause issues with breaking continuity with patients and potentially increasing their length of stay. Workloads can also be unbalanced if other factors are not accounted for such as patients that have not been seen overnight.
What Are the Benefits and Challenges of Continuity of Care Rounding?
Many of the hospitalists we have worked with like to consider themselves the patient’s PCP in the hospital. They don’t want to transfer the care of their patient to someone else while they are on service. Continuity of care is better for the patient and the provider. Numerous studies have shown that increased continuity of care increases patients’ satisfaction, patient safety and reduces length of stay. Each transition of care that occurs from one provider to another requires knowledge transfer and a ramp up of the provider’s knowledge of that patients stay within the hospital. Handoffs in their nature take additional time but also have multiple variables that lead to complexity, such as the acuity of the patient and the current care plan that is being followed but also how these specific patients and their families interact with the care providers.
In the patient assignment process, continuity of care provider should be a focus point.
As with geographic rounding, continuity appears to be a simplistic form of patient assignment:
- As a Hospitalist, when I’m assigned a new patient, I will follow them through their entire hospital stay.
- The inevitable handoff to another physician when the current attending goes off service.
- If a patient is still in the hospital when the original attending comes back on service, the assignment returns to the original attending.
- Patients may be in multiple different locations within the Hospital.
- The outcomes of consistently rounding on this patient will outweigh all the inconveniences that come with getting passed along to another Hospitalist.
- Developing a relationship with the patient and/or their family is important because I’m the one who’s aware of the patient’s medical history.
- If this patient is readmitted in the future, having myself assigned to this patient would be ideal because of the rapport and knowledge we already have with one another.
- Their stay at the hospital becomes much easier on them and me because of the relationship that had been previously established.
Problems arise when only trying to employ continuity between providers and their assigned patients through the entirety of their stay. The biggest challenge is for larger hospitals that may have multiple floors and/or multiple towers. If only continuity is being considered for patient distribution, providers may be traveling large distances back and forth to see their patients which may increase response time to patient in delivering care and add to provider burnout. Also, having patients in multiple locations makes multi-disciplinary rounds difficult/impossible.
How Do You Build a Hybrid Patient Assignment Model That Works?
The most optimal outcome we have seen is create a hybrid model that leverages the best functions between the two while also considering other assignment factors to evenly distribute patients.
A clear way to create a balance between geographic rounding and continuity to create a geographic region that is honored before that patient is transferred to another provider. For example, if a patient moves more than two floors away or even to a different tower, that patient is then re-assigned to a provider within the other geographic “bubble”. Length of stay can also be a factor to determine who to keep on your rounding list and which patient should be reassigned to another care provider. Creating a balance between the two will give your hospital the best of both worlds. Also, if my unit is full and the unit next to me is not, the provider working the unit next to mine can take some of my workload.
A hybrid model will create better balanced provider workloads with the result of having better outcomes for the patients. Studies have shown, if you manage continuity and workloads, you get lower LOS, lower readmission rates, and higher patient satisfaction. Combining geographic rounding with continuity is also a physician satisfier. The Hospitalists will know where they are working for the most part on a given day and can be sure that there is logic in place when transferring their own patients over to other care providers.
Implementing a geographic and continuity hybrid patient assignment methodology is a difficult task to do with a manual system. Even beyond geography and continuity, there are a wide range of different variables that creates increased complexity with each one added. This ranges from the different attributes of the patients in the hospital census to the actual structure and individual characteristics of the providers working any given day. The work at a hospital also never ends, which means this is a process that is typically done with a large patient distribution happening in the morning but then also throughout the day.
We have seen the key to success is to fully understand all these variables and how they interact and ensure that the solution is configured based upon the desired outcomes for the hospital, providers, and patients. This consultative approach along with the transparency of the distribution methodology creates confidence that the best possible outcomes is reach every time.
Table 1: Geographic vs. Continuity vs. Hybrid Patient Assignment Models
Conclusion
While optimizing infusion billing and charge capture ensures hospitals aren’t leaving revenue behind, another key challenge lies in hospitalist efficiency and continuity of care. One area where hospitals often struggle is geographic rounding — when physicians are assigned patients scattered across multiple units. This leads to wasted time, more handoffs, and physician burnout.
By predicting where ER patients are likely to be admitted, hospitals can assign them as if they’re already in their destination unit. This proactive approach, made possible through tools like Medaptus Assign, integrates with Epic’s pre-assignment or bed request features to map patients to the right hospitalist before they leave the ER. Customers like Texas Health and Rochester are already using this strategy to preserve geographic rounding, reduce inefficiencies, and strengthen the doctor-patient relationship.
Just as automated infusion charge capture closes revenue gaps, predictive hospital bed planning closes workflow gaps. Together, these strategies empower hospitals to align financial, operational, and clinical goals — ensuring revenue integrity, physician satisfaction, and most importantly, better patient care.
FAQs
Is Geographic or Continuity Rounding Better for Patient Outcomes?
Research shows continuity of care leads to better patient satisfaction, safety, and lower length of stay. However, pure continuity creates travel burden and physician burnout in larger facilities. The hybrid model — using a geographic zone as the trigger for patient reassignment — delivers the patient outcomes of continuity with the efficiency of geographic rounding.
How Far Should a Patient Move Before Being Reassigned to a New Physician?
A common threshold is two or more floors away, or a move to a different building or tower. The specific rule should be configured based on your hospital’s layout. medaptus Assign allows this threshold to be customized as part of your rules engine.
Can medaptus Assign Implement a Hybrid Assignment Model Automatically?
Yes. medaptus Assign’s rules engine is specifically designed to automate hybrid models — enforcing geographic zones, respecting continuity where possible, balancing workloads, and updating assignments throughout the day as patients move. This removes the manual burden from charge nurses and list-makers.
What Outcomes Have Hospitals Seen with a Hybrid Assignment Model?
Studies show that managing both continuity and workloads together produces lower length of stay, lower readmission rates, and higher patient satisfaction. Additionally, physicians report higher job satisfaction when they can predict their rounding geography while trusting that patient transfers follow a logical, fair process.

About The Author
Malachi Charbonneau is the Chief Executive Officer of medaptus, where he leads the company’s strategy, growth, and innovation in healthcare revenue cycle and workflow automation. Since joining medaptus in 2011, he has held leadership roles across client implementation, customer success, sales, and operations, giving him deep expertise in healthcare technology and provider workflows.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.











