

Blog Summary
Physician groups lose revenue at three predictable points: incomplete charge capture, claim denials that age without action, and patient balances that never get followed up on. This post breaks down what’s actually in your accounts receivable, where the gaps tend to show up, and how medaptus helps physician groups turn accounts receivable into predictable revenue.
I’ve been on a lot of calls with physician group administrators over the past few years. There’s a sentence I hear so often: “We know we’re leaving money on the table. We just don’t know where.”
Sometimes it’s $50K. Sometimes it’s closer to $500K. But the feeling is always the same. The care was delivered. The physicians did their jobs. Somehow, the revenue didn’t follow.
Accounts receivable (A/R) isn’t a glamorous topic, but for physician groups managing complex payer contracts, mobile providers, and patients, getting it right is everything. So let’s talk about where the money actually goes.
What Does Physician Accounts Receivable Actually Include?
A/R is everything your group is owed for care already delivered but not yet paid. That sounds simple until you start mapping it out.
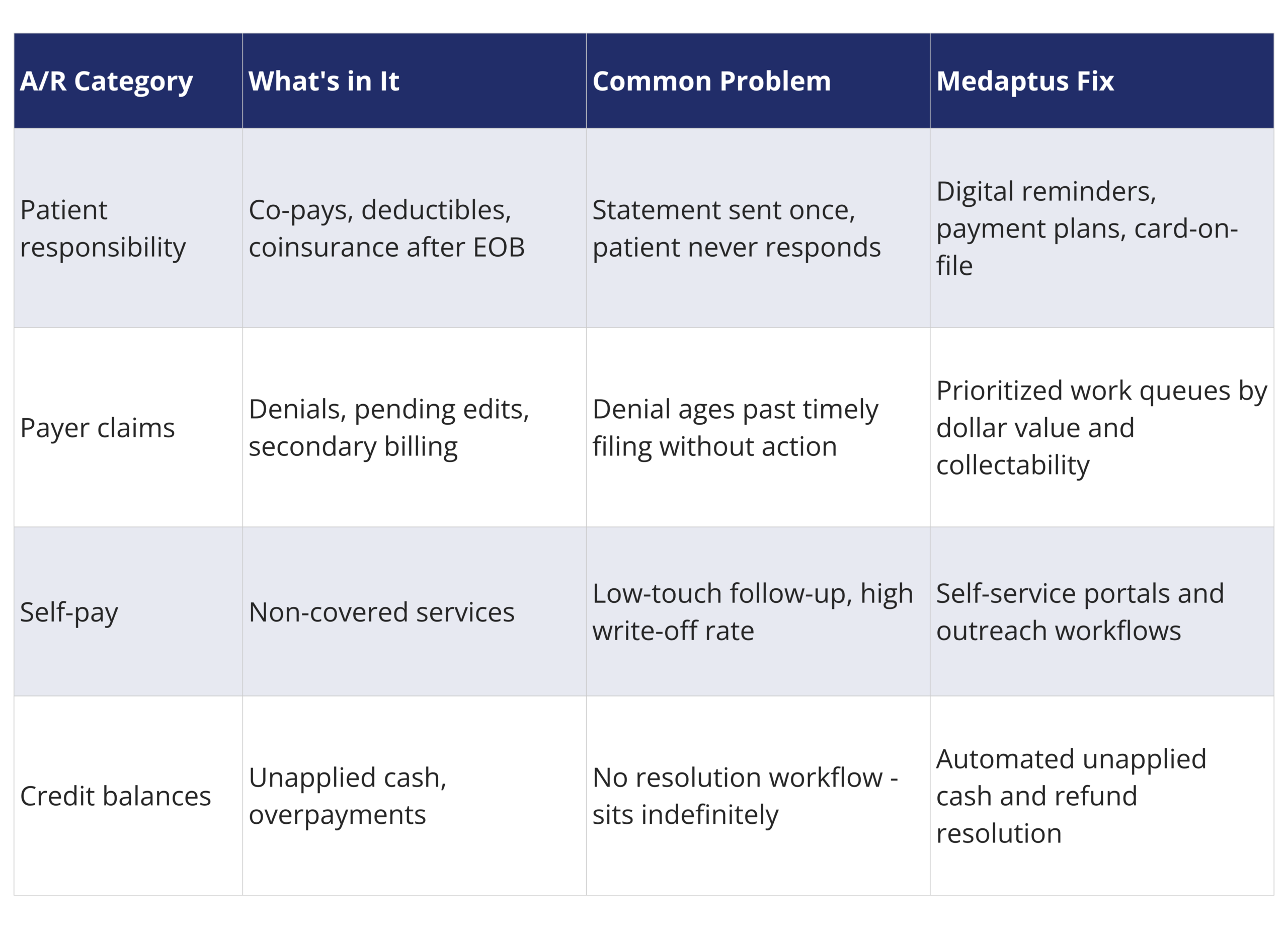
A/R spans patient balances after insurance adjudication (co-pays, deductibles, coinsurance after the EOB), payer claims in edit hold or waiting on secondary billing, self-pay amounts for non-covered services, and residuals from coordination of benefits issues that never got resolved. Most physician groups are managing all of these categories simultaneously, across multiple payers, locations, and specialties, meaning they need a pain-free system for document integration as well. Groups that handle both professional and facility medical billing are managing that complexity across two billing tracks at once. It compounds fast, and so does the risk of money slipping through.
Where Does the Revenue Actually Go?
In my experience, the leaks are almost always in the same three places.
- Charge capture. If a physician submits a charge late, submits it incomplete, or doesn’t submit it at all, everything downstream starts at a disadvantage. This is especially common with mobile providers and hospitalists who are documenting between patients on the go.
- The claim level. Denials that don’t get worked quickly age past timely filing. Payer rules that weren’t applied at submission create rework. And when work queues aren’t prioritized by dollar value and collectability, your team ends up spending the same effort on a $40 claim as a $4,000 one.
- Patient collections. A single statement mailed to an address that may not be current, with no follow-up and no easy way to pay, is not a collections strategy. Patients will pay when the process is clear, convenient, and timely. Most of the time, it isn’t.
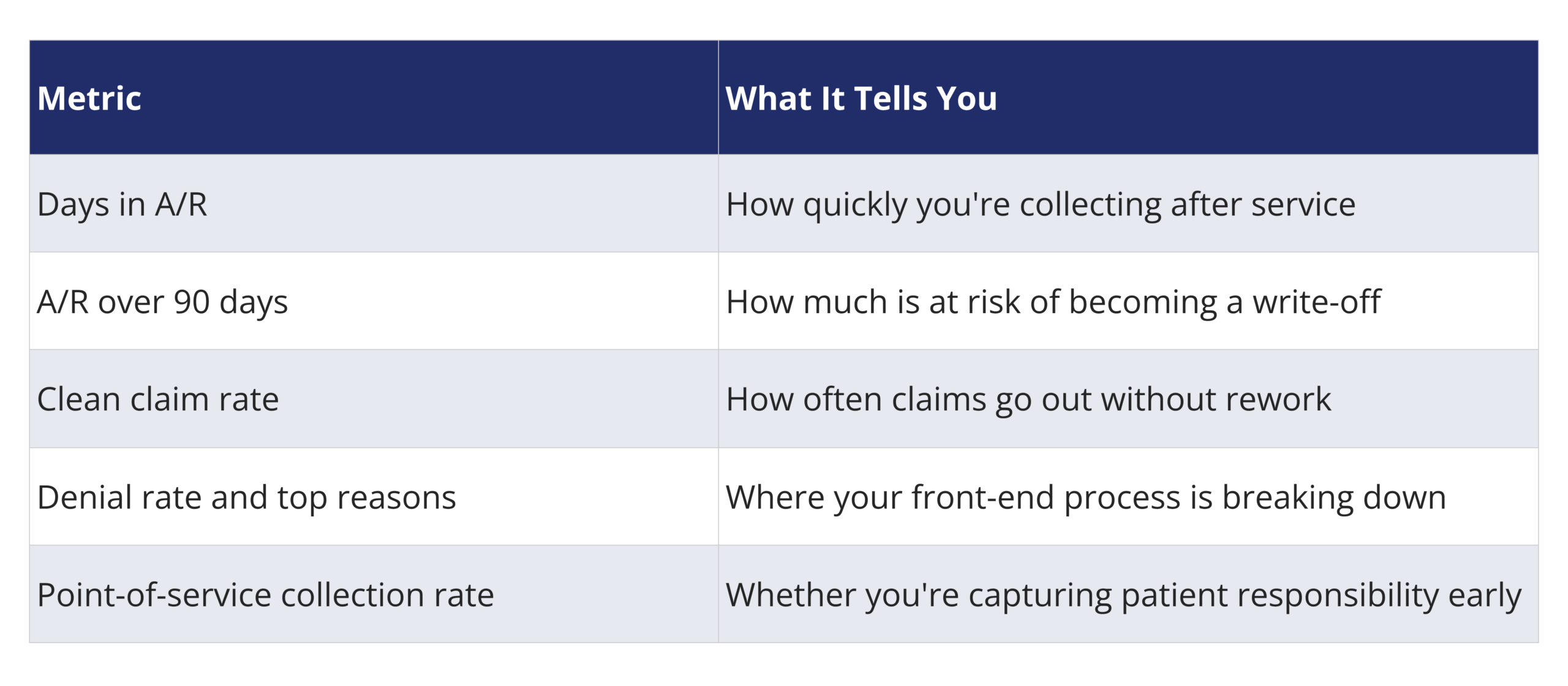
What Should Physician Groups Actually Be Tracking?
If you want to know whether your A/R is healthy, these are the five metrics that matter most:
How Does medaptus Help Physician Groups Close the Gap?
Medaptus approaches the physician revenue cycle as a connected workflow from the moment a charge is captured to the moment the payment posts. We work with the hospitals you partner with to ensure all necessary patient information syncs to the medaptus Charge Pro system.
Charge capture starts at the point of care. Physicians submit through mobile charge capture for physicians with real-time edits and payer-specific rules applied at entry. By the time a claim goes out, the obvious issues are already caught. Automated reconciliation then compares documentation, encounters, and charge status to find gaps before they become denials.
Physician data management keeps provider, location, and specialty information consistent across payer contracts and billing systems. Errors here create downstream headaches that take weeks to unwind, and most billing teams don’t catch them until the denial shows up.
On the patient side, medaptus supports clear statements, digital reminders, payment plans, and card-on-file options that make it easier for patients to pay. The goal isn’t just a better collection rate, but rather making the process less confusing for patients, which happens to accelerate cash too.
Work queues for the billing team are prioritized by collectability and dollar value, so the highest-impact items get worked first, every time.
Physician A/R at a Glance
Conclusion
If you’ve noticed that money is leaving your organization and you just can’t tell where, it’s almost always a process problem. And process problems are fixable.
The question worth sitting with: at which point in your revenue cycle does your visibility actually break down? Charge capture? Claim submission? Patient follow-up? That’s where to start.
We’re happy to walk through where medaptus fits in your current workflow. Learn more about Charge Pro.
FAQs
What does physician accounts receivable include?
Patient balances (co-pays, deductibles, coinsurance after the EOB), payer balances in edit hold or under appeal, self-pay amounts for non-covered services, and credit balance residuals from unapplied cash or overpayments. Most physician groups are managing all of these at once.
What are the most common causes of physician claim denials?
Missing or incorrect provider information, payer-specific rules not applied at submission, and late charge capture are the most frequent culprits. The fix usually starts at the front end, before the claim goes out.
How does mobile charge capture for physicians reduce A/R days?
By applying edits and payer rules at the point of entry, charges go out cleaner and claims require less rework. Fewer denials means faster payment and fewer write-offs.
How do you reduce A/R over 90 days?
Prioritize work queues by dollar value and collectability, address denials quickly after receipt, and follow up on patient balances through multiple communication channels rather than a single mailed statement.
Does medaptus replace our billing system?
No. Medaptus integrates with existing billing systems and EHRs. It adds the workflow layer (charge capture, reconciliation, data management, and collections) that most billing systems weren’t built to handle on their own.

About The Author
Vicky Abihsira is the Director of Sales and Marketing at medaptus, where she leads the company’s market strategy and business development initiatives. She specializes in connecting hospitals and health systems with solutions that improve revenue cycle outcomes and clinical workflows.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.











