

Blog Summary
Nurse-patient assignments are one of the most critical — and most overlooked — drivers of patient safety, quality of care, and nurse satisfaction. Research shows 76% of nurses learned to make assignments from colleagues or self-taught, and 74% know someone who transferred or left due to assignment-related unhappiness. Studies confirm that well-balanced, computerized nurse-patient assignments improve patient safety, reduce errors, and increase job satisfaction. Yet most hospitals still rely on manual, untrained charge nurses to create assignments without viable decision-support tools.
As hospitals continue to try to reduce costs, improve operations and still provide quality care, one area that might benefit from an evidence-based practice review could be nurse-patient assignments. There’s certainly no shortage of complaints and concerns about the process among nursing units.
Whether it’s concerns about favoritism leading to unfair nurse-patient assignments or whether it’s heavy workloads leading to frustration and burnout – nurse workloads and how they are created are gaining attention. Even the training behind them is under scrutiny.
What Does Research Tell Us About How Nurses Learn to Make Assignments?
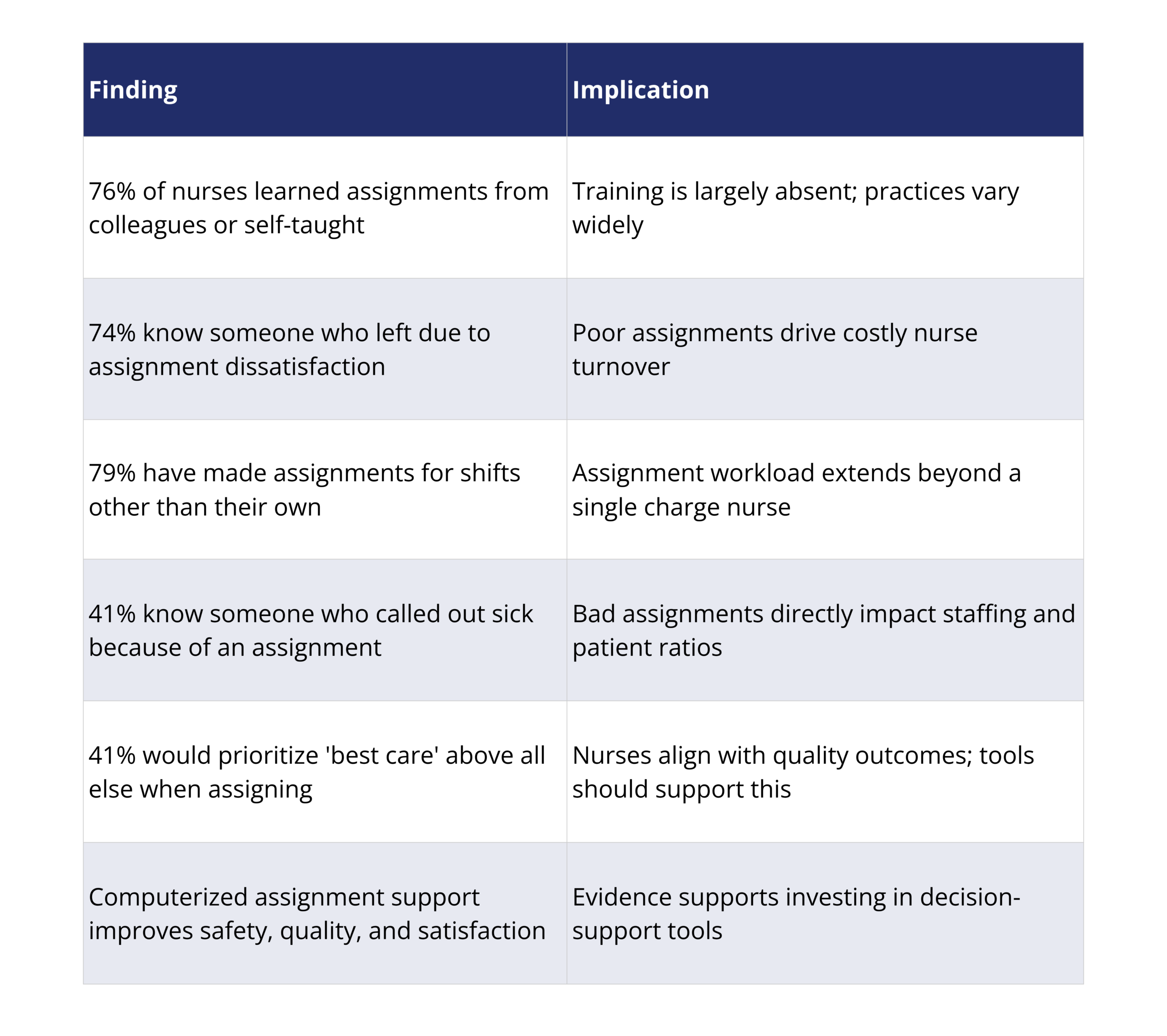
In a limited study of 58 nurses, researcher Stephanie Allen of Pace University asked a group of nurses how they learned to make nurse-patient assignments. Six percent of the respondents said they learned in their primary undergraduate program, while another 9 percent said they got formal hospital training. But three out of four respondents (76%) said it was a colleague or learned on their own.
In addition, 9 out of 10 of the nurses surveyed said they had at some point made a nurse-patient assignment and the majority of them indicated that they began making assignments within 2 years of graduating from nursing school.1
Perhaps more alarming, 74% of the nurses surveyed said they knew someone who transferred or left their position because of unhappiness with their nurse-patient assignments and almost all of them said that their daily nurse-patient assignment was extremely or very important to their overall job satisfaction.
Some other interesting findings from this particular study:
- 79% of the respondents said they made assignments for a shift other than their own
- 41% of nurses knew someone who called out sick because of an assignment
- 41% said if they could choose only one purpose when making assignments, it would be “best care”
What Are the Implications of How Nurse-Patient Assignments Are Made?
What are the implications of this study and others related to workload and nurse-patient assignments?
There’s still much work to be done.
Whether it’s the result of insufficient nurse-patient ratios or cost-cutting measures, the evidence has been building that heavy nursing workloads can adversely affect the delivery of care. In addition, there’s also compelling evidence to suggest that matching the right nurse to the right patient in the “right environment” can lead to positive quality and safety outcomes. In another study where a computerized decision support system (CDSS) was implemented to assist nurses and nursing teams with their daily, recurring nurse-to-patient assignment process, the researchers concluded that creating well-balanced, high-quality assignments is crucial to “ensuring patient safety, quality of care, and job satisfaction for nurses.”2
And yet, almost all nurse-patient assignments today in most hospitals are done manually and backed with little or no training. Patient acuity tools haven’t proven to be all that helpful either. While some EHR systems and patient classification systems have been moving towards trying to attach some kind of coding or numbering system to different acuities, problems surface.
Table 1: Key Findings from Nurse-Patient Assignment Research at Pace University
Why Do Current Patient Acuity Tools Fail Nurses?
It’s not unusual for a patient acuity classification system coming out of the EHR to be more geared towards physicians and their needs instead of the needs of nurses, which makes it either unusable or cumbersome to try to customize.
Then there’s the problem of patient acuity or classification systems specifically geared towards nurses. They might be able to code a patient’s condition and allow for a charge nurse to assign a particular nurse based on that coding. But it still doesn’t take into account a host of other factors that need to be considered when trying to match the right nurse to the right patient. For example, what about geography AND patient acuity? How can those two be balanced?
Furthermore, what if you want to also try to factor in continuity? Now, instead of using just one criteria – patient acuity– you’re suddenly dealing multiple variables at once in a maddening juggling act that challenges even the most savvy and experienced nurse.
Imagine the difficulties of this patient-assignment task on a nurse with one to two years of experience. With little or no training and no viable tools, charge nurses and others are left to come up with balanced, fair and meaningful workloads at a time when budgets continue to be tightened and greater care is not only asked for, but demanded.
Conclusion
Maybe it’s time to take a fresh look at nurse-patient assignments — especially since it can be argued, and the evidence supports it, that they are one of the pillars of quality inpatient nursing care. The solution lies in decision-support software that accounts for multiple variables simultaneously: geography, continuity, patient acuity, workload balance, and skill matching. Without such tools, charge nurses — regardless of experience — are being asked to do the impossible.
FAQs
Why Do Poor Nurse-Patient Assignments Lead to Nurse Turnover?
Research shows 74% of nurses know someone who left or transferred because of assignment unhappiness, and 41% know someone who called out sick because of a specific assignment. When nurses feel their assignments are unfair, overly burdensome, or disconnected from best-care principles, job dissatisfaction builds — and turnover follows.
Do Patient Acuity Systems Solve the Nurse Assignment Problem?
Not fully. EHR-based acuity systems are often designed for physician workflows, not nursing. Even nurse-specific acuity tools typically use a single variable — patient condition — and don’t balance it with geography, continuity, or workload equity. Effective nurse-patient assignment requires optimizing multiple variables simultaneously, which requires decision-support software.
What Does Research Say About Computerized Nurse Assignment Support?
Studies show that a computerized decision support system (CDSS) for nurse-to-patient assignments creates well-balanced, high-quality assignments that improve patient safety, quality of care, and job satisfaction for nurses. The research concludes these outcomes are difficult to achieve through manual processes.
What Variables Should a Nurse-Patient Assignment System Account For?
An effective system should factor in patient acuity, geographic proximity to the nurse’s primary unit, continuity (keeping the same nurse-patient relationship across shifts where possible), workload balance across the nursing team, and individual nurse skill sets and certifications. Balancing all these simultaneously requires purpose-built software.
1 Assignments Matter: Results From a Nurse-Patient Assignment Survey. Stephanie B. Allen, PhD, MSN, MS, BSN, ASN. Lienhard School of Nursing, College of Health Professions, Pace University, Pleasantville, NY. 44TH Biennial Convention, Sigma Global Nursing Excellence
2 Developing and testing a computerized decision support system for nurse-to-patient assignment: a multimethod study. van Oostveen CJ1, Braaksma A, Vermeulen H.Comput Inform Nurs. 2014 Jun;32(6):276-85. doi: 10.1097/CIN.0000000000000056.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.











