

Blog Summary
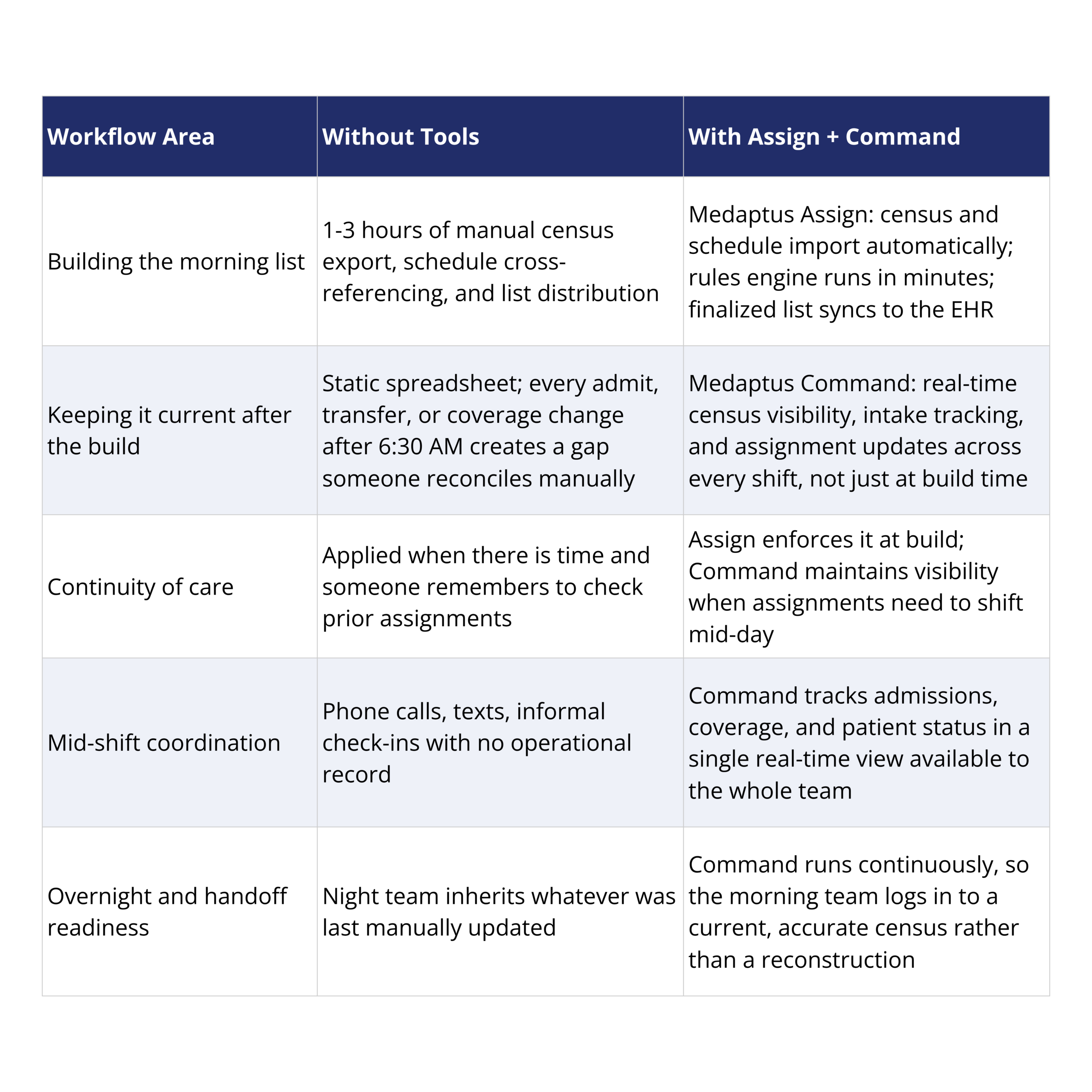
Most hospital medicine programs have two rounding assignment problems, not one. The first is the morning build, a manual process that takes 1-3 hours and produces a list that coordinators and providers work from to start the day. The second is what happens after: the census changes, patients are admitted and transferred, coverage shifts, and the rounding list does not update itself. This piece walks through what solving both problems actually looks like, with medaptus Assign handling the morning build and medaptus Command handling the real-time operational picture that takes over once rounds begin.
One of the things I hear most often from hospital medicine coordinators when I talk to them is some version of the same thing: the morning assignment takes a while, and then it tends to become outdated quickly after that.
I think about that a lot, because both halves of that sentence are problems, and they are different problems. I have found that most programs are only thinking about the first one.
The time cost is real. Most programs are spending 1-3 hours every morning manually pulling the census from the EHR, sorting patients by geography, figuring out continuity, checking the provider schedule, and distributing the result by text or email or whatever works. At Northwell Health’s South Shore University Hospital, that number was three hours every morning before they started using medaptus Assign, and it dropped to 10 to 15 minutes after.
But the second half of the problem is the part that tends to get absorbed quietly without anyone fully accounting for it. The rounding list you build at 6:30 AM is accurate at 6:30 AM. By 9:00 AM, a patient has been admitted from the ED, someone has transferred, a provider handed off coverage at shift change, and the list does not know any of that. Someone has to reconcile the difference, either by updating the spreadsheet or by providers figuring it out as they go. It is coordination overhead that was not in the original time estimate, and it compounds throughout the day.
So there are really two things to solve here, and they need different tools.
Part 1: Solving the Morning Build
Why is it so hard to let go of the manual process?
I get why programs stick with it. It works well enough most mornings. The list gets built, rounds happen, patients get seen, and the day moves forward. The problems are incremental and they distribute across the team in ways that do not always show up as a single clear failure. The coordinator is on the phone reconciling assignments. A provider gets two patients they were not expecting. Continuity of care slips on a high-volume morning because there was not time to check prior assignments carefully. None of those are catastrophic on their own.
What makes it hard to see is that the manual process has always worked just well enough that nobody questions it. The assumption is that this is just how rounding assignment works, that some amount of coordinator time in the morning is inherently required, and some amount of reconciliation throughout the day is just part of the job.
It is not. That is the actual reason I wanted to write this.
What does automated rounding assignment actually look like?
I think ‘automated’ can sound like a black box, so I want to be specific about what the process looks like with medaptus Assign, because it is more practical than the word makes it sound.
There are four steps, and your coordinator is still in the loop for all of them.
Step 1: Import the patient census. The census pulls directly from your EHR, no manual export, no copy-paste from a printout, no downloading a file and uploading it somewhere else. The data reflects where things actually stand at the time of import.
Step 2: Import the provider schedule. This pulls from whatever physician scheduling software you are using, or you can upload a file if needed. The system knows who is available, when their coverage starts, and what role they are in.
Step 3: Run the rules engine. This is where the logic that coordinators are already applying manually every morning gets defined once and applied consistently every time. The four rule categories are:
- Continuity of care, meaning assigning the same providers to the same patients across consecutive days where possible
- Provider handoff and succession, which maintains ownership through shift changes
- Geographic grouping, which clusters patients by floor or unit to reduce rounding time
- Patient attribute weighting, which factors in acuity and complexity for workload distribution.
Your team defines the logic, and the system applies it the same way on a 40-patient morning as it does on a 20-patient morning.
Step 4: Finalize and distribute. The coordinator reviews the output, makes any manual overrides, finalizes the list, and distributes it. The finalized assignments sync back to the EHR, so everything lives in one place and providers see their assignments in the system they are already using.
The whole process takes under 30 minutes. For most programs it is 10 to 15 minutes. And because the logic is defined once and runs consistently, the morning build does not vary based on who is doing it or how much time is available, which is where manual processes tend to fall apart on high-volume days.
That is Part 1 solved. But as I said at the start, there are two problems.
Part 2: Solving What Happens After the List Is Done
This is the piece that I think gets underestimated, and it is the one I want to spend more time on here, because it is what we have been hearing about from programs and thinking hard about on the product side.
Assign builds a great list. It is balanced, it reflects continuity, it is organized by geography, and it takes 15 minutes instead of three hours. And then rounds begin, and the day happens.
A patient comes in from the ED at 8:15. A transfer from the ICU lands on the floor. Someone’s coverage shifts at noon. By mid-morning, the rounding list is a historical document. It shows what the assignments looked like at 6:30, not what they look like now. And there is no system keeping track of what changed.
The coordinators and providers absorb that gap themselves. Phone calls to figure out who owns a new admit. Informal check-ins to confirm who is still covering which patients. A coordinator manually updating a spreadsheet in real time, which works until it does not. None of this is tracked anywhere, and none of it is visible to anyone outside the immediate conversation.
What Medaptus Command Does Here
Medaptus Command is what we built to address what happens after the morning assignment is done. It is a hospital medicine operations platform that keeps running throughout the day, tracking new admissions as they come in, maintaining visibility into who owns which patients, managing coverage transitions, and giving the whole team a shared, real-time view of where things stand.
The way I think about it: Assign handles the build. Command handles the day.
When a new patient comes in from the ED, Command captures the intake. When coverage changes, Command tracks it. When the morning list starts drifting from reality as the census shifts, Command is the system that keeps the operational picture current, so providers are not piecing it together from phone calls and coordinators are not manually reconciling a spreadsheet against what they are hearing from the floor.
And it runs overnight, too. The night team works from a live operational picture, not whatever was last manually updated before the evening coordinator went home. The morning team logs in to a census that is already current, which, as it turns out, also makes the Assign build faster, because the data they are starting from is accurate.
The two products are designed to work together, and that is intentional. Assign solves the inefficiency in the morning build. Command solves the operational gap that opens up the moment the list is done. Assign itself will actually be a tab within Command so customers of both products can view everything in one platform.
Conclusion
The thing I find most interesting about this, having talked to a lot of programs that have made the switch, is that the time savings with Assign are immediate, but what tends to matter more to people over time is the consistency. The morning build does not vary based on who is doing it or how busy it is. Continuity of care does not get skipped when the census is high. The coordinator still makes judgment calls, but they are making them on top of a solid baseline instead of building from scratch every morning.
And then Command picks up where Assign leaves off. The operational picture that Assign establishes at 6:30 AM stays current throughout the day, so the coordination work that currently falls on people, the phone calls, the manual updates, the informal check-ins, moves into the platform instead.
If you are curious what the implementation looks like for your specific EHR setup, that is a conversation worth having sooner rather than later. The integration piece is a lot more straightforward than most programs expect.
Learn more about medaptus Assign
Learn more about medaptus Command
FAQs
What are the two rounding assignment problems most hospital medicine programs have?
The first is the morning build, a manual process that takes 1-3 hours and produces an initial rounding list. The second is what happens after: the census changes throughout the day and the static rounding list does not update, so coordination gaps accumulate across every shift.
What does medaptus Assign solve?
Assign solves the morning build. It imports the patient census from the EHR and the provider schedule from your scheduling software, runs a rules engine for continuity, geography, succession, and patient attributes, and produces a finalized rounding list in under 30 minutes. Northwell Health’s South Shore University Hospital reduced their daily build from three hours to 10-15 minutes.
What does medaptus Command solve?
Command solves what happens after the morning list is done. It tracks new admissions, maintains real-time census visibility, manages coverage transitions, and gives the whole team a shared operational picture throughout the day, so coordination does not fall back on phone calls and manual spreadsheet updates once rounds begin.
Do Assign and Command work together?
Yes. They are designed to complement each other. Assign handles the morning build efficiently; Command maintains the real-time operational picture for the rest of the day and overnight. Both integrate with your EHR.
Does using Command mean we do not need Assign?
They solve different problems. Command gives you real-time operational visibility throughout the day, but the structured, rules-based morning build that Assign provides, with its continuity logic, geographic grouping, and workload balancing, is still the right tool for creating the initial rounding list efficiently.

About The Author
Jaclyn Corbett is the Product Manager for medaptus Command and Assign, with over 13 years working at the intersection of healthcare operations and software development. She works directly with hospital medicine programs to understand how operational workflows break down and how technology can reconnect them.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.











