

Blog Summary
A successful hospital patient assignment software implementation depends on organizational readiness. Hospitals that assign IT resources early, observe existing workflows before configuration, validate rules using real production data, and provide structured post-go-live support typically complete implementations faster and achieve higher user adoption. Most implementation delays stem from unprepared IT teams rather than technical limitations, while ongoing support after launch helps clinical teams build trust in the new workflow, reduce manual assignment time, and improve operational efficiency.
When using our smart assignment software, medaptus Assign, providers barely notice because every patient landed on their MDR list automatically. Everything starts working as it should. No more manual cross-checks, no more morning scramble. One hospitalist operations lead described it as patients appearing on the list “with a flick of a button.”
That was the good news from a customer after recently going live on medaptus Assign.
The friction came later. And it didn’t come from the software.
After nearly 15 years running healthcare technology implementations, I can tell you: the technology is almost never the hardest part. The hard part is what happens between a system that’s technically ready and a team that’s operationally ready to trust it. That gap exists in every go-live. How wide it gets, and how fast you close it, depends on what you do before, during, and after launch.
Here’s what that process actually looks like.
Why Does an Implementation Take 60 Days at One Site and 90-Plus at Another?
There’s never been a situation I’ve been in where the client wants to move faster than us. We have the resources, we’re staffed, and we’re ready to go.
Where we’re going to see delays is when an IT staff either wasn’t fully informed or notified or ready to go at signature. They’re kind of scrambling to figure things out. There’s no project manager assigned. No hours scoped. No budget allocated. Compare that to the implementations that move fast: a great project that moves quick has the IT team already staffed. There’s a project manager, and each role is already filled and ready to go.
Assign is interface-heavy by design. We work directly with the EHR, pulling an inbound HL7 ADT census feed, integrating with scheduling platforms like Amion, and writing the attending assignment back to Epic or Cerner.
When a customer gets IT resourced and organized upfront, 60 days is realistic timeline. When there is a communication gap and they figure out about the software change after the purchase, implementation will take 90-plus days.
The fix is simple, but it has to happen before you even purchase a new software: Who specifically on your IT team owns this project? What’s the timeline for their internal kickoff? Do they have hours budgeted? That conversation, early, changes the whole implementation trajectory.
What Steps Are Necessary to Prepare for a Go-Live?
Companies like to build software around a clean model: one attending in, one attending out. But hospitals rarely run that clean. You have continuity rules (keep the same attending for a 30-day readmit), geo-rounding rules (cluster patients by floor to reduce travel time), and load-leveling rules (balance census across providers). Those layers have to be sequenced in a way that reflects how the clinical team actually prioritizes decisions.
Step 1: Observe Current-State Workflows
The most important thing I do before touching a single configuration setting is observe current-state workflow.
Even a session or two watching how a team actually runs morning assignments tells me things no intake form will surface. At one recent Epic go-live, we discovered late in implementation that the site was using dummy provider codes more extensively than I’d initially scoped.
“With our teaching teams, we use dummy codes for our residents. In order for that resident to have a flag on the patient chart, they have to be listed as the attending. But we also have to have one of the hospitals listed as the attending. “
— Hospitalist Operations Lead
They also had patients carrying more than one attending. That’s something they admitted came from being an early Epic adopter. These were institutional habits that had never been formally documented. Now they’re on my discovery checklist for every Epic client.
Step 2: Performing a Parallel Run
After observing current state, the next move is getting production data flowing as early as possible, before go-live. Some teams call this a soft go-live or pre-go-live. I call it a necessity. Real patient data lets us test real scenarios, troubleshoot rules in real time, and run a parallel: seeing what Assign would have done side-by-side with what the team did manually, then tuning from there.
One thing I tell every clinical lead going into parallel: the goal is confidence. Parallel testing validates that the system handles your most common scenarios correctly, and it consistently does. But chasing every edge case in a test environment before going live is a cycle that doesn’t end. Going live is what accelerates learning. The system performs well. The faster you’re in it for real, the faster your team builds the confidence to trust it.
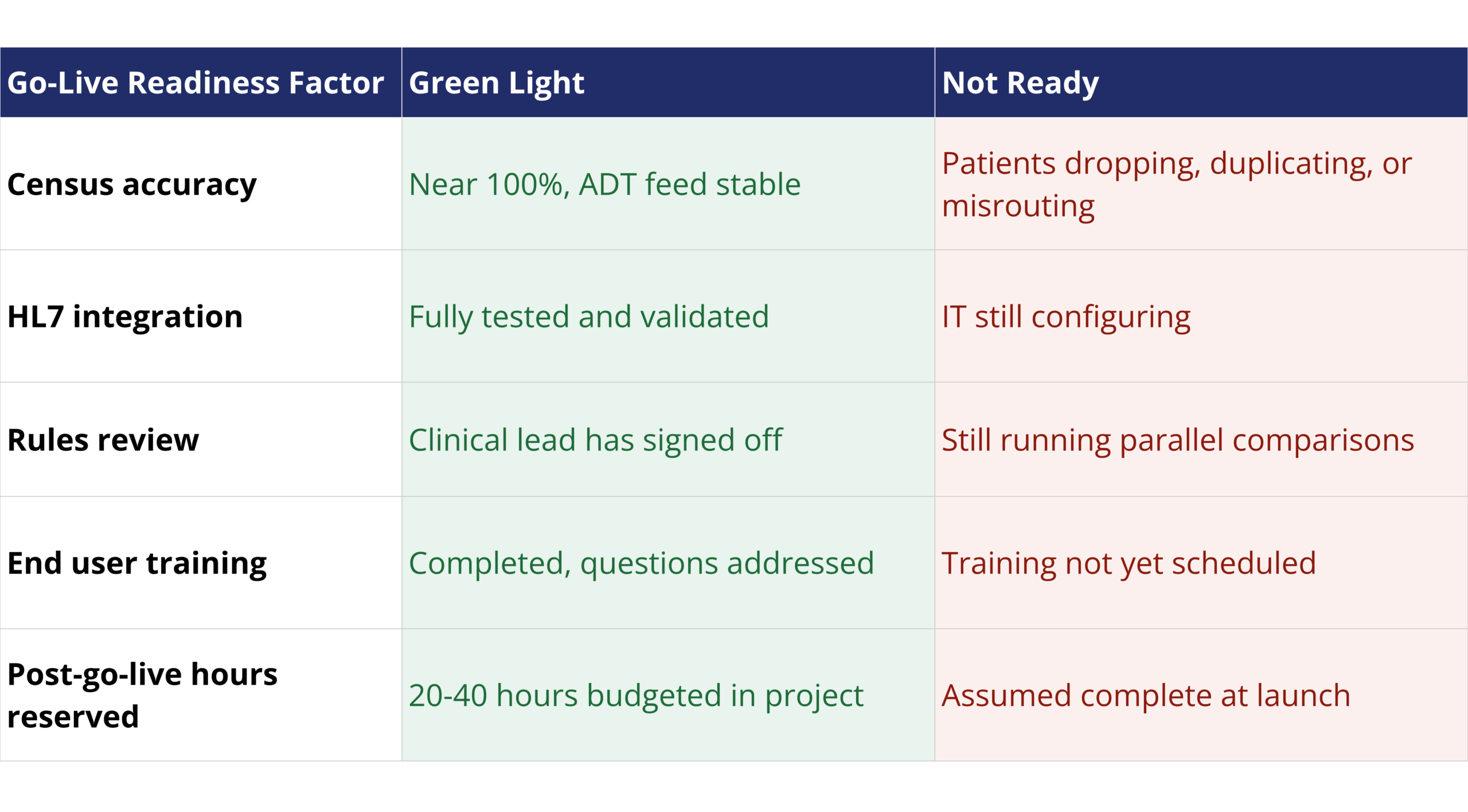
When Do You Know It’s Actually Time to Go Live?
Two things have to be true before I’ll call a site ready.
First: census accuracy must be as close to 100% as possible. If the ADT feed isn’t clean, with patients dropping off, duplicating, or misrouting, we don’t go live. Census issues require coordinating between two interface teams to resolve. Census is my hard gate.
Second: sign-off on the rules. I want a few review sessions with the clinical lead, looking at actual system output against actual census scenarios. Once they see what Assign produces and agree it reflects how they want to operate, we’re ready.
Rules can be tweaked quickly after go-live. Census problems cannot. That’s why I sequence it that way.
The system is ready before most clients feel ready. That’s normal. Some nuances only surface in live use, and that’s fine, because rules can be updated quickly. The goal is a confident go-live.
What Post-Go-Live Actually Looks Like
Go-live is not the finish line.
Go-live is not the finish line. There’s almost always a couple of weeks of significant hands-on support after launch. Some people are surprised by that. They think go-live means we’re done. But there are two leading indicators I like to watch to measure success: time savings and issue volume.
Time savings: Before Assign, how long did morning assignments take? At sites running Assign at full adoption, teams consistently complete morning assignments in 20 to 30 minutes. That efficiency gain is the ROI we deliver. In the early weeks post-launch, I track whether that trend is moving in the right direction as a signal that the workflow is clicking and users are trusting the system.
We dive into the nuances immediately: Is it end user behavior? Something misconfigured? What’s different here from other recently live sites getting assignments done in 20 minutes? Usually the answer is workflow compliance, with users reverting to manual steps instead of trusting the system.
Issue volume: Our team likes to stay on post-go live to support your staff as they learn to use the new assignment system. The goal here is to learn how you work. Something I listen for is if anyone is discussing the same issues on repeat. That tells me something is structurally wrong. I bring in the right people, whether that’s IT, rules review, or more user-level support. We are always on call in real-time to make sure the system meets your expectations and that your staff understand the new workflows. At one recently live site, the hospitalist operations lead described the tech literacy gap plainly:
“Teaching somebody to copy and paste from one Excel sheet to the other took three days. If that tells you how much we had to take a step back, it was a lot that I was not prepared for personally.”
That’s not a knock on the staff. It’s a reality of who ends up running patient assignment software in some organizations. Long-tenured nurses starting at 4 a.m. They were trained to be nurses, not computer users. When you hand them a tool that feels different from anything they’ve touched before, the learning curve isn’t about the software. It’s about trust.
As for the end users who follow the process. The results speak:
“Today was the first day that we were done on time because we trust the process and all of our bumps were mostly gone… all my patients are on my MDR, which is not something we have routinely had. So that was really great.”
— Hospitalist Operations Lead
That’s the outcome we’re building toward. It just takes a few more weeks to get there than some clients expect. That’s where post-go-live support earns its value. We stay close, build troubleshooting guides for common scenarios, and keep chipping away at the edge cases until the team doesn’t need us anymore.
Conclusion
Successful go lives come down to a few things that are knowable and controllable: having IT resourced and organized before day one, taking time to actually observe how the team works before configuring anything, and getting real production data in play early.
The technology will do its job best when we work together to set up the conditions where the people can trust it.
That’s what we focus on at medaptus, not just building the integration, but being there through the parts where it gets complicated. If you’re planning an Assign implementation and want to talk through what that process should look like for your environment, let’s connect.
FAQs
How long does a typical medaptus Assign implementation take?
Most implementations land between 60 and 90 days. The biggest factor is IT resourcing, specifically whether the client’s IT team has a project manager assigned, hours scoped, and budget allocated at or before signature. When those are in place, 60 days is achievable.
What interfaces does Assign require?
Assign integrates with your EHR to receive an inbound HL7 ADT census feed, connects to scheduling platforms (such as Amion) via API, and writes the attending assignment back to your EHR, whether that’s Epic, Cerner, or another system. This is interface-heavy work, which is why IT readiness matters so much upfront.
Do you need production data before going live?
Yes. We require a production feed before go-live, not to launch, but to test real scenarios, run parallel comparisons, and troubleshoot rules before clinical staff are depending on the system. Some teams call this a “soft go-live.” I call it a non-negotiable part of the process.
What’s the most common reason a go-live gets delayed?
IT resourcing, by a wide margin. A client whose IT team wasn’t fully informed or ready at signature will consistently fall behind. Clinical teams are usually ready to move. The bottleneck is almost always on the technical side.
How much support should we expect after go-live?
Plan for two to four weeks of significant post-launch support. We budget 20 to 40 hours of post-go-live time within our project scope specifically because of this. Go-live is when real use-case edge cases surface: rules behavior in live scenarios, user adoption patterns, and IT-related issues that weren’t visible in testing.
What if our end users didn’t choose the software?
This is more common than you’d think. When a system is mandated rather than requested by the end users, there’s a salesmanship component to implementation that goes beyond training. We focus on the “why” alongside the “how,” and we design training to meet users where they are, including users with lower technology comfort levels or shift structures (like 4 a.m. starts) that affect how and when they engage.

About The Author
Jeff Cibotti is a Senior Solutions Consultant at medaptus with nearly 15 years of experience in healthcare technology. He specializes in hospital medicine workflow, patient assignment automation, and EHR integration.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.











