
Blog Summary
Most hospital medicine tools were only built for the morning assignment. After rounds end, admissions keep coming, census changes, and providers manually fill the gaps through calls and spreadsheets. True continuous operations requires five core workflows — intake, assignment, census visibility, distribution, and overnight readiness — running in real time across every shift, not just at 7 AM.
It’s 6:45 AM.
The attending logs in to start rounds. The census from overnight is somewhere in a shared folder. Three new admissions are pending – two from the ED and one from a referring team. Nobody has been formally assigned yet.
She starts making calls.
This is how hospital medicine begins for a lot of programs. Not in chaos but in reconstruction. Before a single patient is seen, the team is already spending time figuring out what the operational picture looks like.
What Does the Research Say About Hospitalist Burnout?
According to a recent study by the Society of Hospital Medicine, nearly 45% of hospitalists report experiencing burnout.
For years, the institutional response has followed a familiar pattern: resilience training, wellness programs, mental health resources. These are not bad ideas. But they do not address what the research increasingly identifies as the root cause of burnout.
Why Is Hospitalist Burnout Often an Operational Problem?
Survey results released by the National Library of Medicine cite unsafe clinical workload as the only factor linked with every measured burnout outcome: emotional exhaustion, depersonalization, diminished personal accomplishment, and low work well-being.
While it is seemingly simple, unsustainable workloads is one of the core issues plaguing hospitalists. And in hospital medicine, workload is often not a staffing problem. It is a coordination problem.
The issue is not how many patients are on the floor. It is how much effort it takes to keep track of all of them.
What Operational Patterns Drive Unsustainable Workloads?
Across hospital medicine programs, four operational patterns consistently contribute to workloads that accumulate beyond what staffing alone can explain:
Operational Pattern |
What It Looks Like |
Why It Accumulates |
| Admissions / Intake | Every new patient arrival creates a decision point: who takes this patient, which team, and which unit. Without a structured intake process, those decisions happen through phone calls, texts, or verbal handoffs. | When volume spikes, the informal system breaks down faster than any individual can manage, creating missed information and delays. It consumes time and creates opportunities for missed information. |
| Distribution / Ownership | Ownership shifts through transfers, coverage changes, and shift handoffs without real-time tracking | When patient transitions are not tracked in real time, providers inherit patients they did not know were theirs, or patients go without a clear owner during the gap. Both outcomes add unplanned work. |
| Patient Assignments | Morning assignment lists reflect the census at one point in time, then drift out of date as admissions, discharges, and transfers occur. | Providers spend time reconciling what the system shows against what is actually happening on the floor, reconstructing the picture multiple times per shift. |
| Reconciliation | Shift-end requires manual cross-referencing of patient lists, nursing confirmation, and discrepancy resolution before sign-out | Administrative overhead compounds at every care transition, consuming time that cannot be spent on patients |
None of these are clinical failures. They are structural ones.
And the people absorbing the gap are the providers.
What Changes When Hospital Medicine Operations Are Coordinated?
When workflows operate independently through calls, messages, and manual reconciliation, the coordination burden falls on people.
When those workflows are connected into a single, real-time operational system, the burden shifts back to the system. A separate 2025 quality improvement study published in the National Library of Medicine has suggested that targeted workflow redesign, like reducing fragmented handoffs, streamlining coordination, and clarifying ownership, leads to measurable reductions in physician burnout scores.
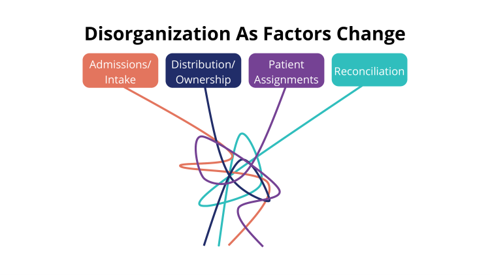
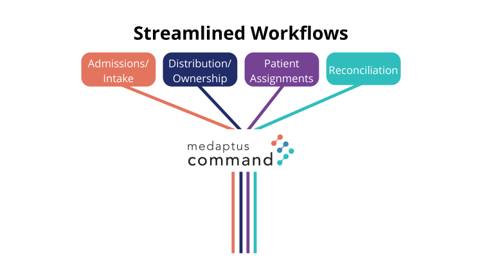 Patient assignments begin the day organized through manual or traditional EHR systems, but grows into an administrative burden throughout the day as factors change. medaptus Command unifies Admissions/Intake, Distribution/Ownership, Patient Assignments, and Reconciliation into a single real-time operational system everyone can view – keeping every hospitalist team aligned as the day evolves.
Patient assignments begin the day organized through manual or traditional EHR systems, but grows into an administrative burden throughout the day as factors change. medaptus Command unifies Admissions/Intake, Distribution/Ownership, Patient Assignments, and Reconciliation into a single real-time operational system everyone can view – keeping every hospitalist team aligned as the day evolves.
What Hospital Medicine Operations Platforms Exist?
Software systems that optimize workflow offer a real point of intervention for reducing burnout and improving hospitalist well-being.
Providers spend less time reconstructing the operational picture. Assignments reflect actual conditions. Intake is tracked automatically instead of manually. This is the environment that reduces burnout: not because the work becomes easier, but because the unnecessary work goes away.
medaptus Command is the hospital medicine operations platform that brings intake, assignment, distribution, reconciliation, and analytics into a single, continuously operating system — reducing the coordination burden that accumulates across disconnected tools and manual processes.
Learn more about medaptus Command →
Frequently Asked Questions About Hospitalist Burnout
Is hospitalist burnout a clinical or operational problem?
Research increasingly points to operational causes. The National Library of Medicine found that unsafe workload was the only factor linked with all burnout outcomes. In many programs, that workload is driven by coordination overhead, not patient volume.
What are the most common operational causes of hospitalist burnout?
Four workflow areas consistently drive unsustainable workloads: Admissions/Intake, Distribution/Ownership, Patient Assignments, and Reconciliation. Without a centralized operational system, each becomes disorganized as the day progresses — creating coordination overhead that accumulates across a shift and consumes time that cannot be spent on patients.
Can workflow redesign actually reduce physician burnout?
Yes. A 2025 quality improvement study found that targeted workflow redesign led to measurable reductions in physician burnout scores. The key intervention was reducing fragmented handoffs and clarifying ownership across the care team.
What is hospital medicine operations software?
Hospital medicine operations software connects core workflows like admissions, assignment, census, patient flow, and analytics into a single system. This replaces the disconnected tools and manual processes that currently create coordination overhead.
How does medaptus Command address hospitalist burnout?
medaptus Command reduces the coordination and administrative burden by connecting hospital medicine workflows in real time. Learn more at medaptus.com/medaptus-command.

About The Author
Jaclyn Corbett is the Product Manager for medaptus Command and Assign, with over 13 years working at the intersection of healthcare operations and software development. She works directly with hospital medicine programs to understand how operational workflows break down and how technology can reconnect them.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.











